Alex Tang
Articles
- General
- Theology
- Paul
- Karl Barth
- Spiritual Formation
- Christian Education
- Spiritual Direction
- Spirituality
- Worship
- Church
- Parenting
- Medical
- Bioethics
- Books Reviews
- Videos
- Audios
- PhD dissertation
Spiritual writing
- e-Reflections
- Devotions
- The Abba Ah Beng Chronicles
- Bible Lands
- Conversations with my granddaughter
- Conversations with my grandson
- Poems
- Prayers
Nurturing/ Teaching Courses
- Sermons
- Beginning Christian Life Studies
- The Apostles' Creed
- Child Health and Nutrition
- Biomedical Ethics
- Spiritual Direction
- Spiritual Formation
- Spiritual formation communities
- Retreats
Engaging Culture
- Bioethics
- Glocalisation
- Books and Reading
- A Writing Life
- Star Trek
- Science Fiction
- Comics
- Movies
- Gaming
- Photography
- The End is Near
My Notebook
My blogs
- Spiritual Formation on the Run
- Random Musings from a Doctor's Chair
- Random Sermons from a Doctor's Chair
- Random Writings from a Doctor's Chair
- Random Spirituality from a Doctor's Chair
Books Recommendation
---------------------
Medical Students /Paediatric notes
Management of Status Epilepticus (in Royal Children's Hospital of Melbourne)
-
Support airway and breathing, apply oxygen by mask, monitor.
-
Secure IV access, check bedside BSL and send urgent specimen for calcium / electrolytes or venous blood gas. If hypoglycaemia present, also seeᅠHypoglycaemia guideline
-
Give benzodiazepine.
-
Repeat benzodiazepine after 5 minutes of continuing seizures.
-
If convulsion continues for a further 5 - 10 minutes, commence phenytoin or phenobarbitone.
-
Consider pyridoxine (100mg IV) in young infants with seizures refractory to standard anticonvulsants.
-
Seek consultant assistance if seizure not controlled.ᅠ Anticipate need to support respiration.ᅠ Thiopentone and rapid sequence induction (RSI) may be required for seizure control.

|
ᅠDrug
|
Route
|
ᅠDose
|
ᅠComments
|
|
Midazolamᅠᅠ
|
IVᅠ
IMᅠ Buccal |
0.15mg/kg
0.15mg/kg 0.5mg/kg (max 10mg) |
IV route preferable but
alternate
routes can be used if rapid IV access not achieved.
If 2 appropriate doses fail to terminate the seizure, further doses are unlikely to be effective and increase the risk of respiratory depression. |
|
Diazepamᅠ
|
IVᅠ
PR |
0.2mg/kg
0.4mg/kg (max 10mg) |
See above, as for midazolam.
|
|
Phenytoin
Phenobarbitoneᅠ |
IV
IVᅠ |
20 mg/kgᅠ
20 mg/kgᅠ |
Both given as loading doses over 30 minutes
in a monitored patient.
|
|
Midazolam Infusionᅠ
|
ᅠIVᅠ
|
Titrate dose
1 - 5 mcg/kg/min |
Incremental increase until control.ᅠOnly to
be initiated in a high dependency setting with involvement
of senior staff.ᅠ May be considered for treatment of
refractory seizures as an alternative to RSI and
ventilation.
|
Taken from Paediatric Protocols for Malaysian Hospitals (2nd Edn)
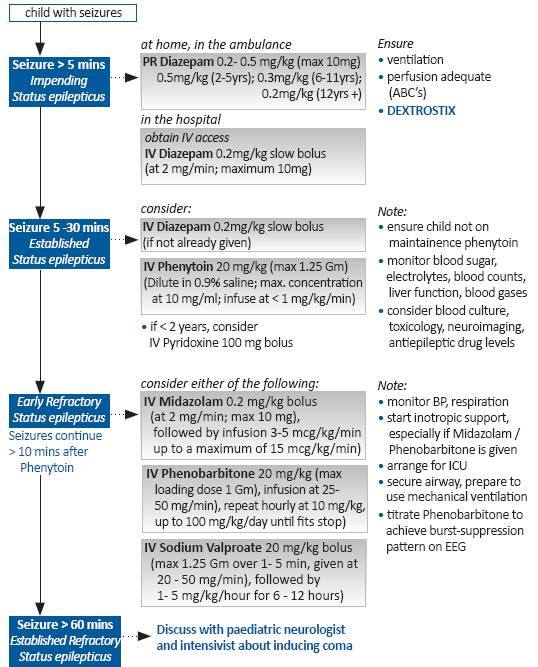
STATUS EPILEPTICUS
• any seizure lasting > 30 minutes or
• intermittent seizures, without regaining full consciousness in between, for >30 minutes
However, any seizure > 5 minutes is unlikely to abort spontaneously, and should be treated aggressively. Furthermore, there is evidence of progressive, time-dependent development of pharmaco-resistance if seizures continue to perpetuate.
Refractory status epilepticus: seizures lasting for >60 minutes or not responding to adequate doses of benzodiazepine and second line medications.
Salient Points
• apart from terminating seizures, management of SE should include, identifying and treating underlying cause
• presence of SE may mask usual signs and symptoms of meningitis or encephalitis, resulting in a danger of overlooking life-threatening infections.
• common mistakes in failing to treat status epilepticus (SE) are under-dosing of anticonvulsant and excessive time lag between doses/steps of treatment
contributed by Ji Keon (Monash)